Monthly Reading List
/
This is my first attempt at a monthly reading list. I plan on making it pretty much the same as the Weekly Reading Lists of the past, only monthly. First, a word about selection criteria ...
The five articles on each list won't be "the best" disability articles I've read, though I'm not likely to post items I think are bad. My selections will be based on a combination of quality, relevance for the month just passed, and content that happens to interest me.
Now, here's the list for June, 2017. All of them are about one topic ... the House and Senate health care bills, especially their implications for disabled people who rely on Medicaid.
Medicaid is My Lifeline
Erin Hawley, Easterseals Blog - June 13, 2017
Erin briefly and efficiently describes in detail how she uses Medicaid-funded home care, and links that to current proposals to cap and cut Medicaid.
Cerebral Palsy Didn’t Stop This College Junior. Obamacare Repeal Might
Jonathan Cohn, Huffington Post - June 17, 2017
This article caught me by surprise. It starts out as a fairly typical story of an inspirational disabled person, almost an inspiration porn story. Then it pivots to show how stories of disability success and virtue also depend on programs like Medicaid that require activism and political support.
Medicaid is a Disability Rights Issue
Erica Mones, Running with Crutches - June 19, 2017
Erica's blog post directly confronts conservative misconceptions about Medicaid ... especially the kinds of casual statements disabled people hear from friends and relatives who should know better, but don't.
Why Disability Rights Activists Stormed Mitch McConnell's Office
s.e. smith, Rolling Stone - June 23, 2017
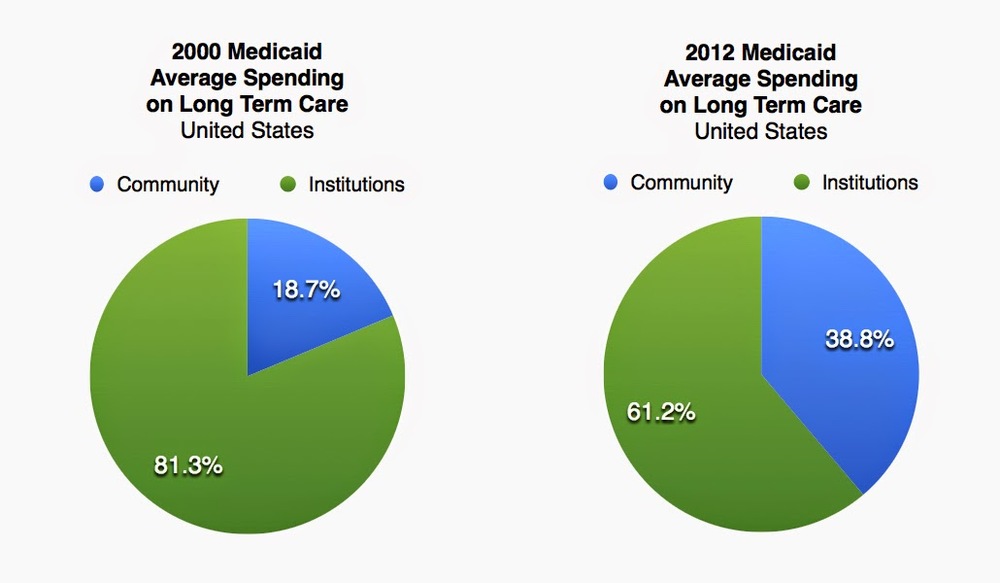
s.e.'s Rolling Stone article connects all the important dots on this issue ... explaining the widely misunderstood links between disabled people, Medicaid, home care, and the struggle to stay out of institutions.
I'm a Republican and I depend on Medicaid
Jonathan Duvall, Pittsburgh Post-Gazette - June 24, 2017
I'm not going to suggest that the same arguments against Medicaid caps and cuts have more validity coming from a Republican, but they may carry a little more weight for conservatives, and with people who speculate that opposition to these proposals is partisan in some invalidating way. Also, I appreciate Jonathan making the point that far from being a ticket to idleness, Medicaid enables disabled people to work. In fact, it's usually a prerequisite to even attempting to work.